
March’s Case of the Month - 2024
Investigating Hypercalcemia in a Geriatric Canine
Patient Information:
Age: 13 years
Gender: Neutered Male
Breed: Maltese
Species: Canine
History:
Patient presented for lethargy and hyporexia. Elevated total calcium was present on laboratory work and confirmed with an ionized calcium. Additionally, renal values were normal. Abdominal ultrasound was recommended with top differential being neoplasia as cause of hypercalcemia.
Abdominal Ultrasonographic Findings and additional recommended diagnostics:
Abdominal ultrasound did not reveal an obvious cause of hypercalcemia. Mild chronic renal changes were present with mild diverticular mineralization (common in hypercalcemia) and mild adrenomegaly was present which was likely attributable to stress response. Given this, a cervical ultrasound was recommended to evaluate for any abnormalities in the parathyroids. Additionally, a PTH and PTHrp level was recommended as well as a rectal exam and 3 view thoracic radiographs.
Left Thyroid gland in sagittal with suspected enlarged parathyroid in the cranial gland.
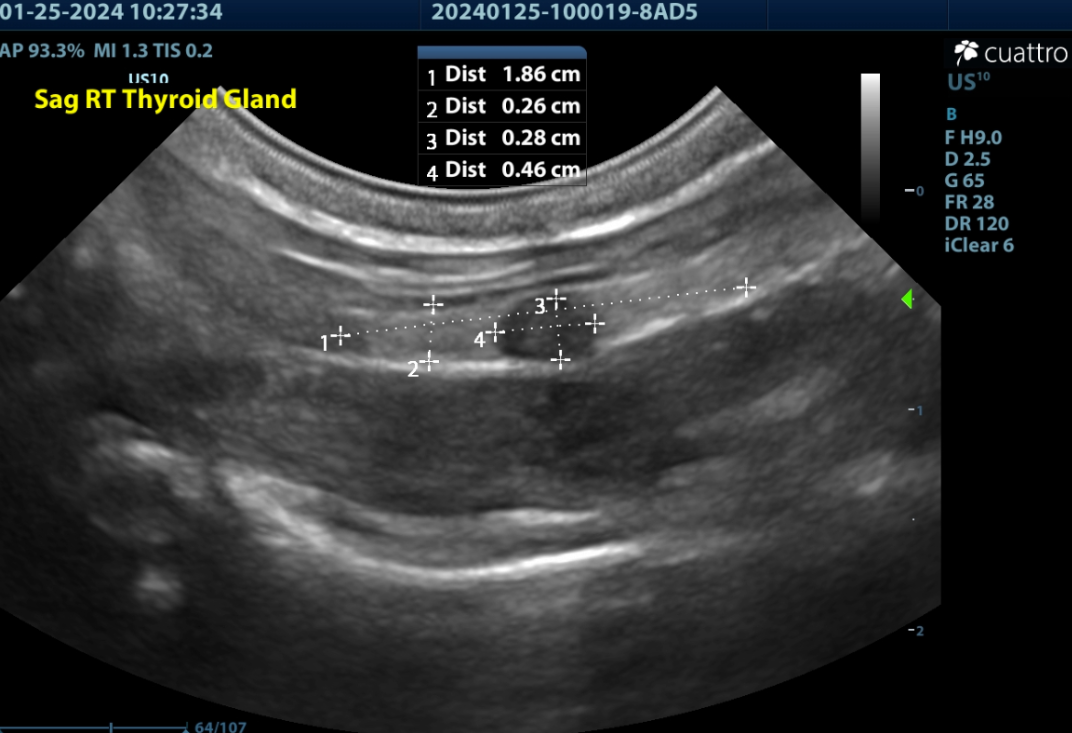
Right Thyroid gland in sagittal with suspected enlarged parathyroid in the mid gland; however, histopathology was consistent with Thyroid C-cell hyperplasia.
Right thyroid gland in transverse with color flow doppler showing the carotid and jugular vessels which are lateral to the thyroid gland. Note how the nodule mildly deforms the normal contour of the thyroid gland.
Left Thyroid Gland in transverse with a rounded hypoechoic nodule consistent with prominent parathyroid gland. Thyroid is located between the heavily shadowing trachea and the partially shadowing esophagus on the left side.

Left Thyroid gland in sagittal with suspected enlarged parathyroid in the cranial gland.
Right Thyroid gland in sagittal with suspected enlarged parathyroid in the mid gland; however, histopathology was consistent with Thyroid C-cell hyperplasia.
Right thyroid gland in transverse with color flow doppler showing the carotid and jugular vessels which are lateral to the thyroid gland. Note how the nodule mildly deforms the normal contour of the thyroid gland.
Left Thyroid Gland in transverse with a rounded hypoechoic nodule consistent with prominent parathyroid gland. Thyroid is located between the heavily shadowing trachea and the partially shadowing esophagus on the left side.
Cervical Ultrasound findings:
The thyroid glands are normal size, shape, and echogenicity. (Lt/Rt WXL=0.3x2.1cm/0.3x1.9cm)
Normal Small Dog Thyroid Length 17-23mm
Normal Small Dog Thyroid Width 3-5mm
There is a prominent homogenous hypoechoic rounded nodule noted in the cranial left thyroid measuring 2.2x2.9mm.
There is a prominent partially contour deforming heterogenous hypoechoic rounded nodule in the mid right thyroid measuring 2.8x4.6mm. Punctate cystic lesions are noted.
Normal Parathyroid Size = 2-3mm
Parathyroid Neoplasia > 4mm (mean of 7mm)
Parathyroid Hyperplasia > 2mm < 4mm (range 3-6mm)
The salivary glands contained punctate hyperechoic foci. (consistent with high calcium levels)
All other visualized structures-lymph nodes, trachea and esophagus are WNL.
Ultrasound Interpretation:
Bilateral thyroid nodules-the findings are moderate-DDx: parathyroid enlargement (diffuse hyperplasia vs. adenoma vs. adenomatous hyperplasia vs. adenocarcinoma) vs thyroid nodule (hyperplasia vs neoplasia)
**parathyroid hyperplasia and neoplasia can overlap in size and cannot be differentiated with ultrasound alone (both look the same sonographically) but requires histopathology to definitively diagnose. Thyroid nodules can also mimic parathyroid gland appearance and also require histopathology for definitive diagnosis.
Recommendations:
A surgical consult was recommended to remove both noted nodules if deemed appropriate at the time of surgery.
Surgical outcome:
The surgery was performed by a board certified traveling surgeon. An enlarged partially cystic nodule was found on the right thyroid. Additionally, the nodule on the left thyroid appeared to be an enlarged abnormal parathyroid gland and therefore was also removed. Both were submitted for biopsy and histopathology.
Histopathology Results:
Tissue submitted as parathyroid gland:
Right: Thyroid C-cell hyperplasia
Left: Parathyroid (chief cell) adenoma
Both were completely excised.
Discussion:
Differentials for hypercalcemia include, neoplasia (lymphosarcoma, apocrine gland adenocarcinoma of anal sac, as well as other carcinomas and select tumors), hypoadrenocorticism, renal failure, nutritional, Vitamin D toxicosis, granulomatous disease and primary hyperparathyroidism (parathyroid adenoma, hyperplasia or adenocarcinoma).
Ultrasonography is a reliable tool for identifying primary parathyroid disease. It has been found to be 90-95% accurate in identifying parathyroid adenomas. The most common presentation is a solitary parathyroid mass (typically adenoma); however, more than one adenoma, adenocarcinoma or hyperplasia can also occur and any abnormal appearing gland should be removed and biopsied at the time of surgery provided at least one functional parathyroid is left to maintain calcium homeostasis. Parathyroid glands and thyroid nodules can appear similar on ultrasound which is why surgical evaluation and biopsy is necessary for definitive diagnosis. Furthermore, it is important to always interpret ultrasound findings in light of laboratory findings. Specifically, PTH, PTHrp, and ionized calcium, BUN/Creatinine/phosphorus and urinalysis are recommended. Hyperplastic glands from secondary hyperparathyroidism (eg renal failure or nutritional) can mimic the appearance of primary hyperparathyroidism. If all 4 parathyroid glands are enlarged, particular care should be taken to ensure that primary hyperparathyroidism is the cause rather than secondary hyperparathyroidism.
Reference: Felman, EC and Nelson RW: Canine and feline endocrinology and reproduction-3rd ed. Philadelphia, WB Saunders, 2004. Pg 689-702.
This case illustrates the importance of identifying and removing any abnormal nodules within the thyroid glands in the face of hypercalcemia (after confirming suspicion of primary hyperparathyroidism as discussed above) and submitting any abnormal tissue for histopathology. Thyroid nodules and parathyroid glands can appear similar on ultrasound as well as grossly during surgery. In this case, the larger nodule was actually not an enlarged parathyroid gland, but a C-cell thyroid hyperplasia due to increased production of calcitonin due to elevated calcium levels. The actual parathyroid adenoma was located on the left thyroid. If only the larger nodule had been removed, then a cure would not have been obtained for this patient.
Case Outcome:
The patient recovered uneventfully from surgery. Initially calcium levels were low, which is common due to the atrophy of remaining parathyroid glands. The patient is currently receiving calcium carbonate and levels have normalized and the patient continues to do well.
Sonographer:
Kara Woody, DVM